In COPD, the DLCO decreases with increasing severity of disease. This is because in emphysema, the lung has lost alveoli, resulting in a lower surface area available for diffusion. In addition, there is also a loss of capillary bed, which can also decrease DLCO.
Is DLCO low in emphysema?
DLCO is reduced in pulmonary emphysema. However, because of the poor distribution of the inspired test gas, the VA may grossly underestimate the TLC, and the resultant KCO may be normal. A reduced DLCO and a reduced KCO suggest a true interstitial disease such as pulmonary fibrosis or pulmonary vascular disease.
Is DLCO affected in COPD?
DLCO is an important factor in exercise intolerance in patients with chronic obstructive pulmonary disease (COPD).
What causes a decrease in DLCO?
There are several conditions that can decrease the DLCO. These include cigarette smoking, emphysema, interstitial lung disease, anemia, decreased lung volume, heart failure, pulmonary vascular disease (pulmonary emboli and pulmonary hypertension), and others.What does it mean if DLCO is low?
Low Dlco less than or equal to 50% predicted can predict hypoxemia with exercise. A normal Dlco does not rule out oxygen desaturation with exercise. Reduced Dlco in the context of normal spirometry, lung volumes, and chest radiographs suggests underlying lung disease such as ILD, emphysema, or PAH.
Why is DLCO decreased in pulmonary hypertension?
A reduced DLco in pulmonary arterial hypertension (PAH) may be the consequence of vascular remodeling and is related to proportionate reductions in alveolar–capillary membrane diffusing capacity and total pulmonary capillary blood volume available for gas exchange.
Why does obesity increase DLCO?
Diffusing capacity and gas exchange An increased DLCO in obese patients is probably related to increased pulmonary blood volume and flow while a decreased DLCO may result from structural changes in the interstitium from lipid deposition or decreased alveolar surface area.
Why does DLCO increase in alveolar hemorrhage?
They may show increased diffusing capacity for carbon monoxide (DLCO) due to increased uptake of carbon monoxide by intra-alveolar hemoglobin; however, this finding, which is consistent with hemorrhage, does not assist with establishing a diagnosis. may be indicated to exclude mitral stenosis.Why is DLCO low in pulmonary fibrosis?
DLCO values represent the ability of the lung to transfer gas from the inhaled air into the blood stream and acts as a surrogate marker of the extent of lung damage (1). DLCO values may decrease because of several clinical conditions including emphysema, interstitial lung diseases, or pulmonary fibrosis (2).
What affects DLCO?The measurement of DLCO is affected by atmospheric pressure and/or altitude and correction factors can be calculated using the method recommended by the American Thoracic Society. Expected DLCO is also affected by the amount of hemoglobin, carboxyhemoglobin, age and sex.
Article first time published onDoes pulmonary edema decrease DLCO?
Background: Heart failure (HF) is often associated with interstitial pulmonary edema and structural changes, resulting in thickening of the alveolar-capillary membrane and reductions in diffusing capacity of the lung for carbon monoxide (Dlco).
What is DLCO in lung function?
A test of the diffusing capacity of the lungs for carbon monoxide (DLCO, also known as transfer factor for carbon monoxide or TLCO), is one of the most clinically valuable tests of lung function. … The DLCO measures the ability of the lungs to transfer gas from inhaled air to the red blood cells in pulmonary capillaries.
Why is DLCO normal in chronic bronchitis?
A decrease in DLCO will be due to a decrease in Va, Kco, or both. Low DLCO and Low KCO: seen in COPD with emphysema due to alveolar destruction (usually normal in chronic bronchitis) with an obstructive pattern on PFT. A normal DLCO with a restrictive pattern on PFT suggests neuromuscular or chest wall disorder.
Why does asthma increased DLCO?
Asthma & DLco The high DLCO values [123, 124] have been explained by hyperinflation, increased intrathoracic pressure, and a more likely cause, increases in pulmonary capillary blood volume or extravasation of red blood cells into the alveolus.
How does smoking affect DLCO?
Even so, smokers can have significantly elevated COHb levels and COHb increases during testing. Elevated PACO and COHb levels will decrease DLCO. PACO back-pressure is estimated to be responsible for about 40% of the decrease and the anemia effect of COHb about 60%.
Why does ERV decrease with obesity?
The most common pulmonary function abnormality in obese subjects is a reduction in the expiratory reserve volume (ERV) (11). This occurs because the mass loading effect of obesity decreases FRC. Because FRC is reduced and the residual volume (RV) is not, ERV declines.
How does being underweight affect three other body systems?
Being underweight can affect your skeletal system. Not getting enough nutrients can make your body calcium deficient, which can lead to osteoporosis (loss in bone density). It can also affect your immune system because your body does not have the nutrients it needs to fight off disease or infection.
How does altitude affect lung capacity?
When living at high altitude for a certain period of time, the human body acclimatizes by increasing pulmonary perfusion and lung capacity, increasing the oxygen-binding capacity of blood and peripheral tissues, and increasing the amount of red blood cells in order to endure the low atmospheric pressure and low partial …
How does pulmonary hypertension affect lung function?
In one form of pulmonary hypertension, called pulmonary arterial hypertension (PAH), blood vessels in the lungs are narrowed, blocked or destroyed. The damage slows blood flow through the lungs, and blood pressure in the lung arteries rises. The heart must work harder to pump blood through the lungs.
Does pulmonary hypertension affect lung capacity?
Spirometry and expiratory flow. 20-40% of patients with IPAH have airway obstruction based on a forced expiratory volume in 1 second to forced vital capacity (FEV1/FVC) ratio of less than 70% [19], [27]. The overall mean FEV1/FVC ratio is significantly reduced at 76% compared to 84% in controls (p < 0.001) [22].
How is low lung volume treated?
Lung volume reduction surgery (LVRS) is a surgical procedure to remove diseased, emphysematous lung tissue. This procedure reduces the size of an over-inflated lung and allows the expansion (growth) of the remaining, often more functional lung.
Is DLCO normal in pulmonary fibrosis?
Conclusions: One in four patients with IPF had normal TLC and more than one-half had a normal FVC during initial evaluation. As the severity of the restriction increased, FEV1⁄FVC increased, DLCO decreased but DLCO⁄VA remained normal.
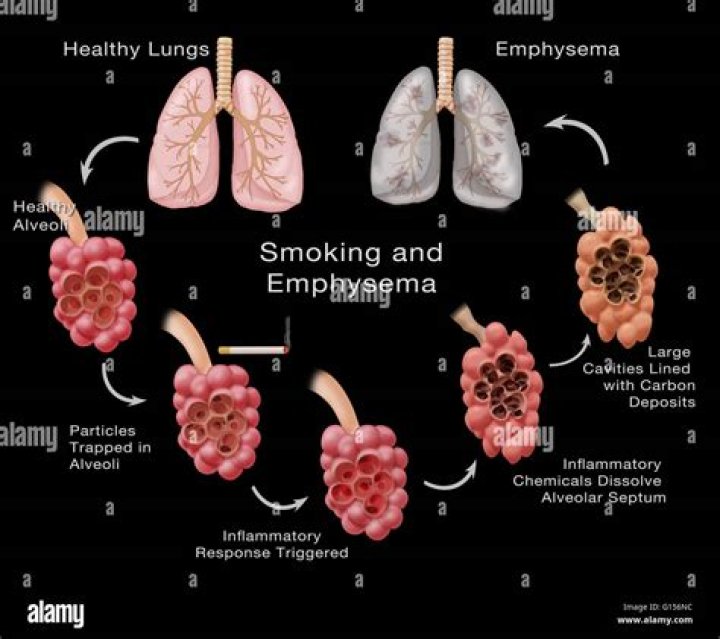
What causes emphysema?
Emphysema is one of the most preventable respiratory illnesses because it is so strongly linked to smoking. Air pollutants, an alpha-1 antitrypsin deficiency, and respiratory infections can also play a role, but smoking is considered the number one cause.
How does hemoglobin affect DLCO?
The impact of an elevated carboxyhemoglobin is twofold: (1) it reduces the alveolar-capillary pressure gradient for CO and (2) acts as a virtual anemia by holding onto sites on the hemoglobin molecule that could be used for binding CO (or oxygen). The net effect is a 2% decrease in DLCO for each 1% increase in COHb.
What is increased DLCO?
Conclusion: A high DLCO on a PFT is most frequently associated with large lung volumes, obesity, and asthma. Other conditions are much less common. A clinical condition, which typically reduces DLCO, may deceptively normalize DLCO in such patients.
How does emphysema affect the diffusion of gases in and out of the lungs?
In emphysema, the inner walls of the lungs’ air sacs (alveoli) are damaged, causing them to eventually rupture. This creates one larger air space instead of many small ones and reduces the surface area available for gas exchange.
Why is alveolar ventilation less than pulmonary ventilation?
Alveolar ventilation is less than the minute volume because the last part of each inspiration remains in the conducting airways and does not reach the alveoli. Similarly, the last part of each expiration remains in the conducting airways and is not expelled from the body.
Why is helium used in DLCO?
During the Dlco maneuver, the 10% helium or 0.3% methane in the test gas enables a single-breath dilution to obtain the Va. The Facoi/Facof indicates the percentage of helium that actually diffuses (or the rate of carbon dioxide transfer and uptake by the Hb).
How does emphysema affect fev1?
A reduction in elastic recoil forces of the lung in emphysema results in several unwanted outcomes. First, airway collapse on forced expiration is accentuated, resulting in a reduced FEV1 and reduced FEV1/FVC ratio, and thus an obstructive ventilatory defect on spirometry.