To limit auto-PEEP, we can try to increase the expiratory time by increasing the inspiratory flow rate and decreasing the plateau time. However, a reduction in inspiratory time and in the ratio of inspiratory to expiratory time may have negative impact on oxygenation, which may not be acceptable.
What causes auto-PEEP on ventilator?
Auto-PEEP occurs in patients receiving mechanical ventilation in the acute stage of acute respiratory failure when they have excessive minute ventilation, resulting in a relatively short expiratory time. This can be explained by the common phenomenon of a time constant in the exhalation phase.
What is a normal auto-peep?
The normal inspiratory to expiratory ratio (I:E ratio) is 1:2. In patients with obstructive airway disease, the target I:E ratio should be 1:3 to 1:4.
What causes high PEEP?
Acute causes of elevated elastic work are pneumothorax, tension pneumothorax, evolving pneumonia, pulmonary edema, ARDS, and auto-PEEP caused by “breath stacking”. Plateau pressures greater than 30 cm/H20 have been implicated in ventilator-induced lung injury (VILI).Which ventilator setting should be changed first for refractory hypoxemia?
Various authors have recommended early (up to 36 h after intubation), high dose prone ventilation (for 12–18 consecutive h/day) as a rescue strategy in patients with severe hypoxemia.
How does Aprv improve oxygenation?
By maintaining a prolonged high pressure (P-high), APRV maximises the recruitment of available lung tissue and therefore improves oxygenation. This is an example of the ‘open-lung’ approach to invasive ventilation.
What is the best ventilation mode for ARDS?
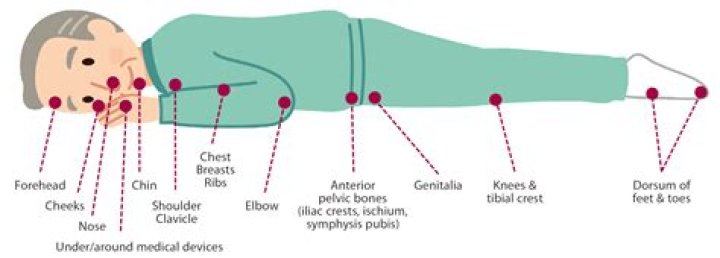
As a treatment, prone position ventilation results in significantly better oxygenation than mechanical ventilation applied in the supine position in ARDS patients [46].
What is the difference between applied PEEP and auto-PEEP?
AutoPEEP= total PEEP – extrinsic PEEP = intrinsic PEEPPEEP= extrinsic PEEP and is preselectedTotal PEEP= intrinsic PEEP + extrinsic PEEPIs ECMO used for ARDS?
Extracorporeal membrane oxygenation (ECMO) can be a lifesaving therapy in patients with refractory severe respiratory failure or cardiac failure. Severe acute respiratory distress syndrome (ARDS) still has a high-mortality rate, but ECMO may be able to improve the outcome.
How do you reduce air trapping?Continuous positive airways pressure may reduce small airways obstruction and therefore air trapping. Pulmonary function tests including lung volumes at rest and and after exercise will be measured. In addition, exercise endurance time before treatment and after treatment will be measured.
Article first time published onWhat is dynamic compliance?
Dynamic compliance describes the compliance measured during breathing, which involves a combination of lung compliance and airway resistance. Defined as the change in lung volume per unit change in pressure in the presence of flow.
How do you fix high peak pressure?
- Increased PIP with normal pPLAT reflects increased airway resistance.
- Reduce airway resistance (suctioning, check ET Tube position, Bronchodilators) Evaluate for Endotracheal Tube obstruction. Consider kinked tubes. Suction for mucous plugs. Consider bronchospasm. …
- Consider increasing the Ventilator pressure limit (caution!)
Does PEEP lower blood pressure?
When PEEP was above 4 cm H2O in the hypertension group, a decrease in blood pressure and ScvO2, and an increase of heart rate were observed. These results indicated that cardiac output significantly decreased.
What is the highest PEEP level?
Under controlled conditions, higher levels of PEEP are well tolerated. PEEP of 29 appears to be the highest tolerated PEEP in our patient. We noted an initial rise in blood flow across all cardiac valves followed by a gradual decline.
How much auto-PEEP is too much?
When used, it is recommended to maintain extrinsic PEEP below 75% to 85% of the auto-PEEP. Again, the use of extrinsic PEEP to treat auto-PEEP has to be driven by strong clinical sense as not all patients will benefit from it and others will be harmed.
Can high PEEP cause pneumothorax?
High PEEP had been reported to be associated with pneumothorax[1] but several studies have found no such relationship[15,17,23,28,37]. Increased pressure is not enough by itself to produce alveolar rupture, with some studies demonstrating that pneumothorax is related to high tidal volume[37].
How is refractory hypoxemia treated?
Clinicians may be required to use a variety of therapies to mitigate life-threatening hypoxemia: high-frequency ventilation (HFV), extracorporeal membrane oxygenation (ECMO), or prone ventilation.
What is the treatment for refractory hypoxemia?
Ventilatory and non-ventilatory strategies that have been used as “rescue” therapies in patients with refractory hypoxemia include lung-recruitment maneuvers, airway pressure-release ventilation (APRV), high-frequency oscillatory ventilation (HFOV), prone positioning, inhaled vasodilators (nitric oxide, prostacyclin), …
What vent mode should be trialed in the case of refractory hypoxemia?
Pressure-controlled ventilation (PCV) is a ventilatory option in cases of refractory hypoxemia, since it can improve hypoxemia without adding further risks–though it does not modify patient survival.
Why is PEEP so high in ARDS?
Positive end-expiratory pressure (PEEP) and fraction of inspired oxygen — The goal of applied PEEP in patients with ARDS is to maximize and maintain alveolar recruitment, thereby improving oxygenation and limiting oxygen toxicity.
How do I set my ARDS ventilator?
The authors recommend initiating ventilation of patients with ARDS with A/C ventilation at a tidal volume of 6 mL/kg, with a PEEP of 5 and initial ventilatory rate of 12, titrated up to maintain a pH greater than 7.25.
Which therapy will be most effective in managing ARDS?
Thus far, the only treatment found to improve survival in ARDS is a mechanical ventilation strategy using low tidal volumes (6 mL/kg based upon ideal body weight).
How do you improve ventilation on APRV?
Increase P-High by 1-2 cm (up to ~30 cm or ~35cm in obesity). T-High manipulation here is a double-edged sword: Increasing T-high may improve recruitment and thereby improve CO2 clearance… if patient is de-recruited. Reducing the T-high will increase the frequency of releases, thereby increasing the minute ventilation.
Can you paralyze on APRV?
Early paralysis is common practice in moderate to severe ARDS patients [45]. However, initiation of paralysis during APRV results in no spontaneous breaths which are analogous to PCV. It is still unknown whether to paralyze a patient versus starting APRV without paralytics for early ARDS.
Is APRV good for ARDS?
It is premature to conclude that APRV is definitely superior to low tidal-volume ventilation. However, this study suggests that APRV is a legitimate front-line ventilator mode for patients with ARDS. Early use of APRV may allow avoidance of paralysis and deep sedation, facilitating more rapid weaning from ventilation.
Why is ECMO good for ARDS?
Initiation of ECMO and the “lung rest” it permits reduce the mechanical power applied to the injured alveoli and may attenuate ventilator-induced lung injury, cytokine release, and multiorgan failure that portend poor clinical outcomes in ARDS.
What is Harlequin syndrome ECMO?
Conclusion: Harlequin syndrome is a known complication of peripheral VA-ECMO, where the upper part of the body is poorly oxygenated. It occurs when the native heart function is preserved but the lungs are poorly functioning. Therapeutic options include converting to central VA-ECMO or VA-V-ECMO.
Why is ECMO used?
ECMO is used when life support is needed after surgery, or when you are very ill and your heart or lungs need help so that you can heal. Your doctor will decide when it may be helpful. If you need ECMO , your doctor and trained respiratory therapists will prepare you.
Is Auto Peep the same as air trapping?
AutoPEEP may also be referred to as air-trapping, breath stacking, dynamic hyperinflation, inadvertent PEEP, or occult PEEP. AutoPEEP is a common phenomenon in mechanically ventilated patients with long expiratory time constants, for example patients with chronic obstructive pulmonary disease or acute severe asthma.
How do you treat air trapping in the lungs?
Your doctor may prescribe a type of medicine called a bronchodilator. It can open up your airways and help reverse the effects of hyperinflated lungs by allowing the trapped air to escape. Certain types of exercise might also help.
What happens when air is trapped in the alveoli?
When emphysema develops, the alveoli and lung tissue are destroyed. With this damage, the alveoli cannot support the bronchial tubes. The tubes collapse and cause an “obstruction” (a blockage), which traps air inside the lungs. Too much air trapped in the lungs can give some patients a barrel-chested appearance.